The COVAX Facility aimed to accelerate the development, production and distribution of COVID-19 vaccines worldwide. To ensure equitable access for 92 low-income (LICs) and lower-middle-income countries (LMICs) within the COVAX Facility, Gavi created a separate funding mechanism — the Advance Market Commitment (AMC). By the end of 2021, the COVAX Facility and AMC had provided close to 1 billion doses to 144 countries. While this vaccine supply was broadly equitable (prioritizing LICs and LMICs), vaccine coverage rates across countries were inequitable. The findings of Itad’s recent evaluation, supported by 3ie, help understand the reasons behind this result and reflect on them for future pandemic preparedness and response.
Evaluation approach
The formative review and baseline evaluation led by Itad focuses on Gavi’s role and examines how the COVAX Facility and AMC performed from its conceptualization in 2020 through to the end of 2021, although it recognizes subsequent relevant shifts till mid-2022. The evaluation is organized through four modules focused on design, implementation, early results and lessons, respectively. As the leader of the "right results" module, 3ie assessed the extent to which outcomes (intended and unintended) and goals were achieved and how the facility and funding mechanism contributed to it by December 2021.
Findings and reflections
The evaluation finds that 87% (833 million) of the 1 billion doses that the COVAX Facility distributed by December 2021 went to AMC participating countries. Thus, the COVAX Facility came very close to meeting its target of distributing 950 million doses to these countries, even though its overall distribution was well below its ambitious target of around 2 billion doses. The COVAX Facility and AMC played a significant role in supplying vaccines to LICs (79% of the supply in 2021), and its contribution was moderate in LMICs (38% without including India) and much lower in non-AMC upper-middle-income and high-income countries (2% and 1.3% of the supply, respectively).
The evaluation also finds that by December 2021, while the COVAX Facility supplied vaccine doses equivalent to covering 22% of the population in LICs with at least one dose, the actual coverage was only 9% during the period. During the same time, LMICs vaccinated around 39% of their population and upper-middle-income and high-income countries more than 70% of their population (see Figure 1). The gap between supply and actual vaccination coverage in the countries that were most reliant on the COVAX Facility was driven by important factors such as the country’s capacity to roll out vaccination, vaccine demand at the time of supply and roll-out, and political will.
Figure 1:Vaccination coverage (at least one dose) over time, by country income group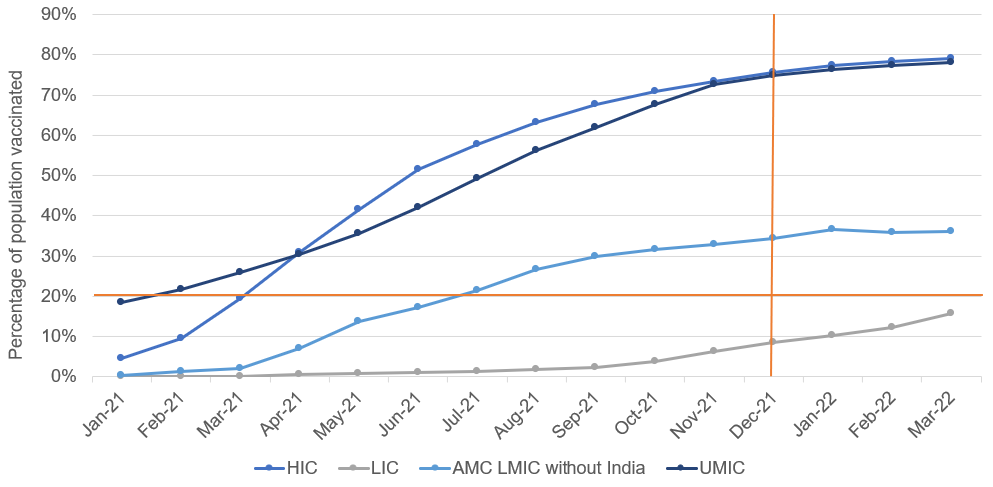
Source: COVID-19 Data Dashboard, https://infohub.crd.co/ accessed August 2022
Inadequate country readiness and capacity to roll out vaccination hampered coverage. On the one hand, there was a general acknowledgment of the value of support from Gavi and other development partners in strengthening country readiness for vaccine roll-out in LICs and LMICs, particularly for cold chain capacity. On the other hand, the evaluation finds that this support would have been more helpful if it had come earlier and if application processes for later rounds of vaccine delivery support had been less burdensome.
The lack of one-to-one mapping between supplies and coverage was also linked to difficulties in aligning vaccine supplies with the demand for doses. The evaluation notes that with the fall in risk perception and misinformation around some vaccine types, community demand for COVID-19 vaccines had reduced by the time deliveries from the COVAX Facility sped up in the last quarter of 2021. Issues with getting doses close to expiry as well as weak political will were also noted as major barriers in LICs and some LMICs.
Ultimately, the results of the COVAX Facility and AMC evaluation show the diverse experience of countries and how the need for support differs dramatically depending on income levels and existing capacity. It also shows that the window of opportunity to act during a pandemic to combat illness, death and cascading economic impacts is very short.
While in this blog we focus on how the results differed by country income levels, the COVAX Facility and AMC evaluation details these and other results in the context of its design and functioning and the evolving COVID-19 crisis. It also highlights critical lessons from this experience, offering recommendations for future pandemic response and aspects of its design, governance and management, supply, allocation and vaccine roll-out. To read a helpful primer on the evaluation, see Itad's article here. To read the report and Gavi's response to it, visit the webpage here. To know more about 3ie's work on immunization, check here or write to info@3ieimpact.org.