A recent BBC article asked why billions of people still lack basic sanitation and they’re not the only ones wondering. According to a 2017 report, 3 in 10 people worldwide (2.1 billion) lack access to safe, readily available water at home and more than 6 in 10 (4.5 billion) lack safely managed sanitation. The water, sanitation, and hygiene (WASH) sector is one of the oldest in international development, with rigorous impact evaluations dating back to the 1970s, but what do we really know? And where does research need to go?
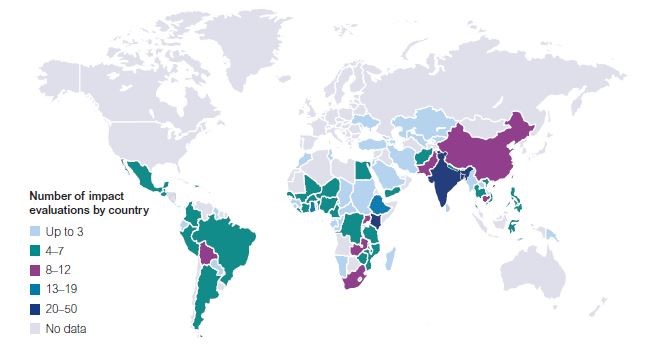
3ie recently produced an evidence gap map for the sector (with accompanying brief and video) which aims to identify, and catalogue, the existing evidence and present it visually. Overall, we found 320 completed rigorous impact evaluations and 42 systematic reviews, with evidence from over 87 countries (see Figure 1), on WASH promotion in households, schools, health facilities, and communities. In addition, we found trial registries and protocols for 47 impact evaluations and 1 systematic review.
Before discussing where we could take WASH research, it’s worth taking a brief look at the evolution of the evidence base. From the 1970s until the mid-2000s, the sector (and therefore the research) was focused on what works. By this we mean which technologies are the most effective at removing pathogens from the environment.
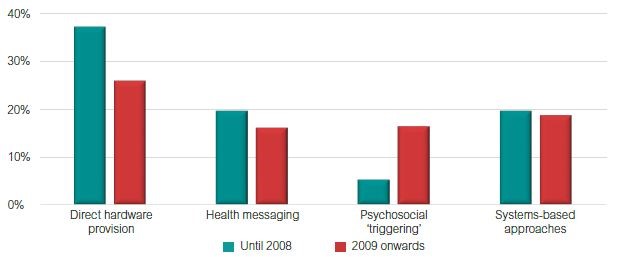
The last 10 years has seen a real shift in the focus of research. As practitioners, policymakers, and researchers began to realise that figuring out what to give people wasn’t sufficient and they also needed to consider how it could be given, a wider variety of intervention mechanisms began to be studied. The biggest shift has been the focus on studying psychosocial triggering mechanisms. These are approaches that leverage social pressure, emotional cues, and other psychological triggers to motivate behaviour change in individuals, and account for nearly 20 per cent of studies in the last decade (see Figure 2).
The most famous of these interventions is community-led total sanitation, which originated in Bangladesh but has spread around the globe.
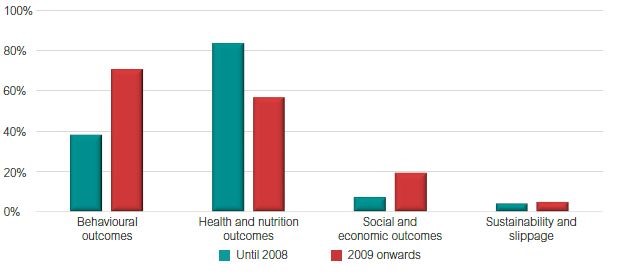
Along with this shifting focus, there has been an increase in the reporting of behavioural outcomes, with over 70 per cent of studies now reporting at least one measure of behaviour (see Figure 3). This is an important change given the increasing understanding that how we provide the same technology (i.e. WASH hardware or practice) might change its uptake and long-term use. Though, having said this, diarrhoea incidence remains the most evaluated outcome. Also, more studies are focusing on sanitation interventions than before, with over 50 completed impact evaluations on them, compared to only 6 studies before 2008, when the International Year of Sanitation brought attention to the area. There has also been a boom in research on WASH in schools.
Going forward, there is still a lot we don’t know and, beyond looking at new, innovative technologies, there are a few gaps (or opportunities) the sector needs to look at if we want to achieve the Sustainable Development Goals (SDGs):
- Gender-transformative (or at least sensitive) programming and evaluations: In an ideal world, this would involve looking beyond the needs of the cis-gendered but, given that only 20 per cent of the studies we identified reported any sex-disaggregated or sex-specific outcomes, first we need to look more at women and girls. Hopefully initiatives like the new female-friendly toilet guide will pave the way, but researchers and practitioners need to consider gender dynamics if we want to encourage equitable solutions.
- More studies on vulnerable populations: We found no studies that looked at (or even captured information on) people living with a disability. We found one rigorous impact evaluation focusing on people living with HIV, two on refugee camps, and one on people living through, or in the immediate aftermath, of a humanitarian crisis.
- Measuring the sustainability of behaviour change: We only found 18 studies that measured a behavioural outcome more than 12 months after the end of an intervention. This is an important step as the effectiveness of interventions may be drastically different when examined in the long-term.
- WASH in health facilities: We identified only one rigorous study of WASH interventions (it was on handwashing) in a health care facility. Given that the WHO estimates that 38 per cent of health care facilities do not have an improved water source, 19 per cent do not have improved sanitation, and 35 per cent do not have water and soap for handwashing, this is also a major gap.
We are hoping that providing this map as a public good will help everyone access the evidence on what works, and help shape research going forward.
These are some of the areas that stood out most as needing further research, but we would love to hear from you on what questions you think the WASH sector needs to be answering? Finally, if you know of any studies you think we have missed, please send them to hchirgwin@3ieimpact.org.









